Login
Welcome back! Please enter your details.
or
Don't have an account? Register here
Create Account
Join MedMentorEdu and start your medical journey.
or
Already have an account? Login here
Enhance your knowledge with our comprehensive guide and curated study materials.
4
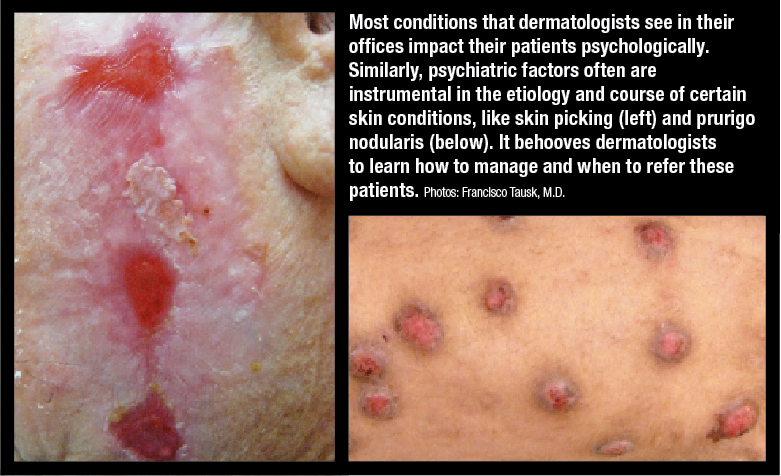
Psychodermatology is a subspecialty that examines the interaction between the skin and psychological conditions.
The skin has been called the "mirror of the mind" due to its connection with stress, emotions, and neurological function.
Patients with psychodermatological disorders often avoid psychiatric clinics, leading to the development of psychodermatology as a distinct discipline.
4
Psychodermatology deals with conditions that lie at the interface of dermatology and psychiatry.
Primary skin disorders influenced by psychological factors
(e.g., psoriasis, eczema).
Primary psychiatric disorders presenting to dermatologists
(e.g., delusional infestation, body dysmorphic disorder).
Psychiatric illnesses developing due to skin disease
(e.g., depression and anxiety following chronic skin conditions).
Coexistence of skin and psychiatric disorders
(e.g., alcoholism with seborrheic dermatitis).



4
Management often requires collaboration between dermatologists and mental health professionals.
A psychodermatology multidisciplinary team (MDT) can improve outcomes.
Dermatologists
Psychiatrists
Psychologists
Dermatology nurses
Pediatricians
Geriatricians
Social workers
Trichologists
Primary care physicians
Patient advocacy groups



4
Different models exist based on collaboration between dermatologists and psychiatrists:
Dermatologist refers to a psychiatrist/psychologist in an external setting.
Remote psychiatric consultation (telemedicine support).
Psychiatrist sits within the dermatology clinic
(most integrated model).
Dermatologist with psychologist as an adjunct provider
(psychologists usually work independently).


4
Classification is complex and relies on DSM-5 (Diagnostic and Statistical Manual of Mental Disorders) and ICD-10/11 (International Classification of Diseases).
DSM-5 provides criteria for psychiatric disorders.
ICD-10/11 classifies all diseases, including psychodermatological conditions.

4
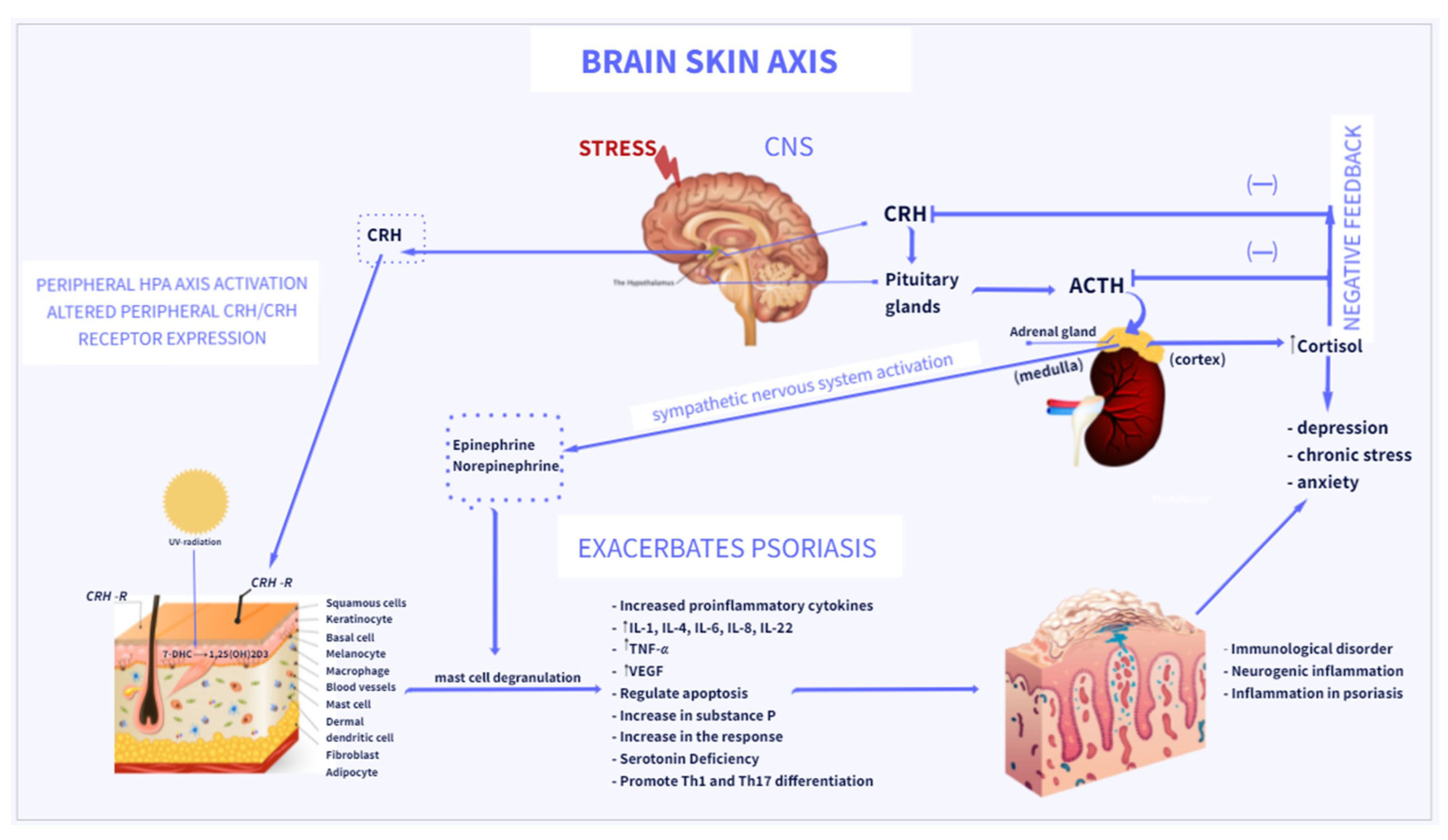
Psychological stress can trigger or exacerbate skin disease.
Mental health assessment should be integrated into dermatological treatment.
Exclude organic disease before assuming a psychological cause.
Treat skin disease and psychiatric illness simultaneously.


4
Skin diseases can cause significant stigma and emotional distress.
Avoidance of social situations
Bullying and discrimination
Reduced self-esteem
Impaired interpersonal relationships
Psychological counseling and support groups
Cognitive-behavioral therapy (CBT) for self-image improvement
Education and public awareness campaigns


4
Chronic skin diseases affect patients' quality of life (QoL), often more than other chronic conditions.
Dermatology Life Quality Index (DLQI)
Skindex-29
Psoriasis Disability Index (PDI)
Psychometric tests can be used to evaluate depression, anxiety, and social impairment in dermatology patients.
Psychodermatology focuses on the relationship between skin diseases and mental health.
MDT approach improves patient outcomes.
Golden rules emphasize treating skin and psychological conditions together.
Stigmatization and quality of life issues require psychological support.
QoL assessment tools aid in patient management.



4
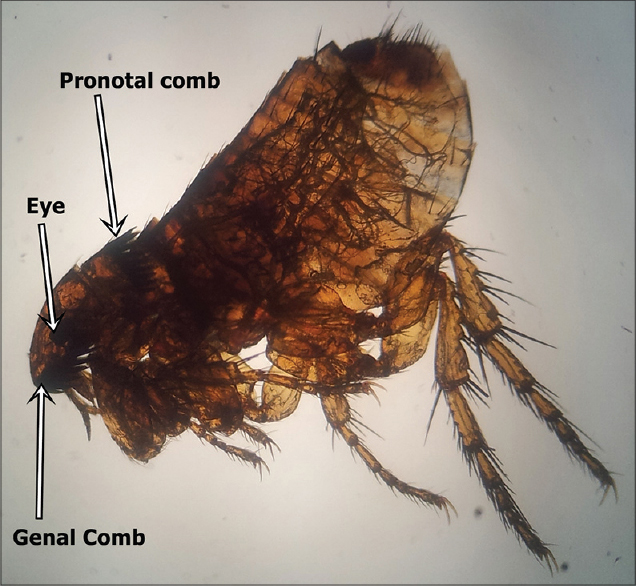
Delusional beliefs are false, unshakeable convictions that arise from internal psychological processes.
These beliefs are not influenced by logic and are inconsistent with the person's cultural and educational background.
Primary delusions
Exist independently
Example: delusional infestation
Secondary delusions
Arise due to an underlying psychiatric disorder
Examples: depression or schizophrenia
Patients may exhibit variable intensity in holding their delusions; some are more responsive to reasoning than others.


4
Also known as:
Ekbom disease
Delusional parasitosis
Parasitophobia
Monosymptomatic delusional hypochondriasis
Patients firmly believe they are infested with parasites, bacteria, insects, or other animate material despite medical evidence disproving their claims.
Estimated incidence: 17 per million people per year.
Peak age: Around 50 years.
Gender distribution: More commonly reported in women
(Male:Female ratio of 1:2.5).
Patients describe sensations of crawling, biting, or stinging.
Patients bring debris, skin particles, or objects they believe are parasites to doctors as “proof.”
Result from excessive scratching, picking, and use of harsh cleaning agents.
Secondary bacterial infections are common.

4
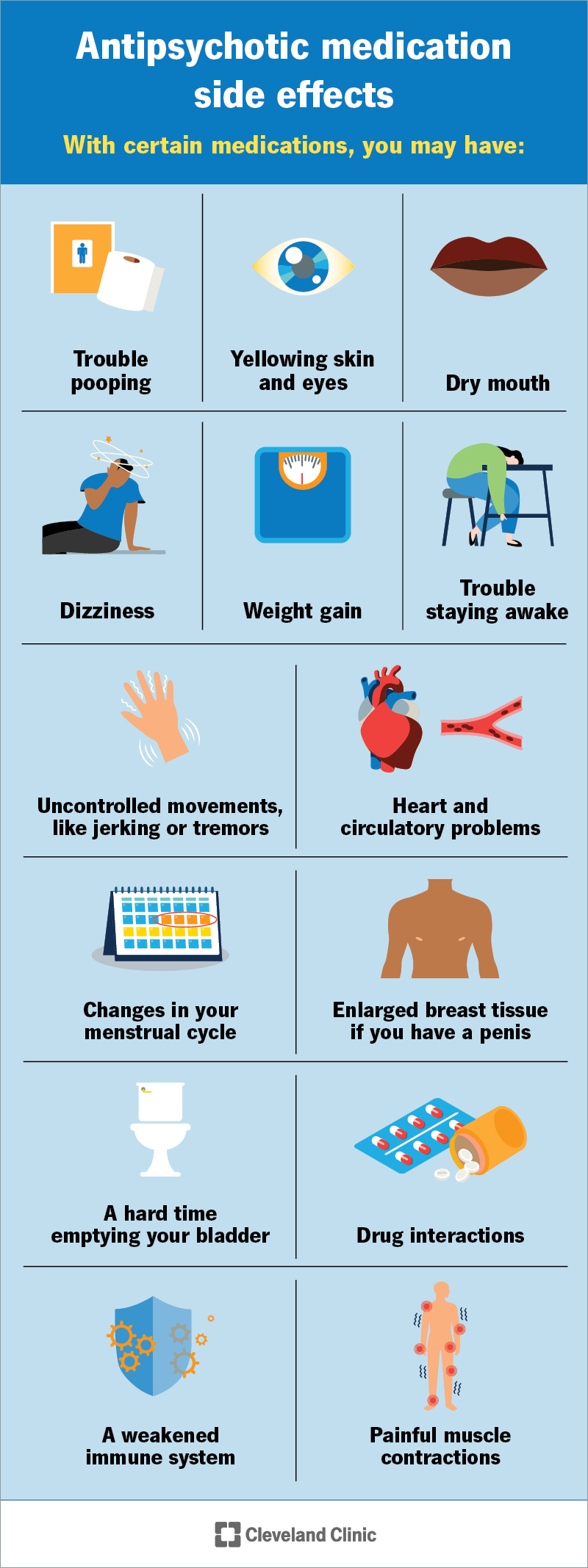
Atypical antipsychotics:
Risperidone (0.5–4 mg/day)
Olanzapine (2.5–10 mg/day)
Quetiapine (25–100 mg/day)
Aripiprazole (5–15 mg/day)
Additional care:
Skin care with antiseptic emollients
Haloperidol or Pimozide (reserved for severe cases)
Tricyclic antidepressants (e.g., Amitriptyline) for associated pruritus
Cognitive Behavioral Therapy (CBT)
(often challenging due to poor adherence)

4
Also called:
Olfactory reference syndrome (ORS)
Delusions of smell
Bromidrosiphobia
Cacosmia
Phantosmia
Patients believe they emit a foul odor, which leads to compulsive washing, social withdrawal, and severe distress.
More common in young men
(Male:Female ratio of 4.5:1)
Can be associated with:
Body dysmorphic disorder (BDD)
Obsessive-compulsive disorder (OCD)
Dementia or temporal lobe epilepsy
Patients report a persistent, unpleasant odor coming from their body, mouth, or sweat glands.
Frequent bathing
Excessive deodorant use
Avoiding social interactions
Patients may become fixated on others’ reactions, for example:
Interpreting someone rubbing their nose as confirmation of their odor.
Depression
Anxiety
Paranoia

4
Selective Serotonin Reuptake Inhibitors (SSRIs):
Fluoxetine
Sertraline
Paroxetine
Additional measures:
Counseling to address compulsive washing habits
Atypical antipsychotics
(Risperidone, Olanzapine in lower doses)
Cognitive Behavioral Therapy (CBT) as an adjunct therapy
4
Morgellons syndrome is a controversial condition in which patients believe that fibers, threads, or foreign materials are emerging from their skin.
Many experts consider it a variant of delusional infestation, although patients strongly attribute the condition to infectious or environmental causes.
Patients report crawling sensations, itching, and skin discomfort.
Presence of fibers or particles in skin lesions, often collected by patients as evidence.
Skin lesions usually result from scratching and picking.
Patients frequently report fatigue, cognitive difficulties, and chronic skin irritation.
Atypical antipsychotics may be used similarly to delusional infestation.
Dermatologic care to treat secondary skin lesions and infections.
Psychological counseling to improve insight and coping strategies.
Delusional beliefs are persistent false convictions resistant to logical reasoning.
Delusional infestation involves a fixed belief of parasite infestation despite lack of evidence.
Olfactory delusions involve belief of emitting foul odors leading to social withdrawal.
Morgellons syndrome is often considered a variant of delusional infestation with reported fibers emerging from the skin.
Management combines dermatologic care, psychiatric treatment, and psychological support.
4
First described in 2001, this disorder is named after a 17th-century description of a hairy skin condition.
Patients believe their skin contains fibers, parasites, or unidentified objects, leading them to obsessively pick at their skin.
It is often linked to delusional infestation, but many patients insist it is a real dermatological condition.
Crawling or stinging sensations under the skin.
Non-healing sores with embedded fibers or granules.
Chronic fatigue, muscle pain, and cognitive dysfunction.
Some patients develop secondary depression or anxiety.


4
The exact cause is unknown, but it is often associated with:
Lyme disease
Substance use disorder
The Centers for Disease Control and Prevention (CDC) found no evidence of an infectious cause, suggesting it is a delusional disorder.


Atypical antipsychotics
Risperidone
Olanzapine
Aripiprazole
Topical antiseptics and systemic antibiotics for secondary bacterial infections.
Phototherapy for skin healing.
Cognitive therapy for behavioral modifications.
Support groups and psychological interventions to address underlying stress and trauma.
Delusional infestation involves false beliefs of being infested with parasites, often leading to severe self-inflicted skin damage.
Olfactory delusions cause patients to obsessively believe they emit a foul odor, leading to compulsive washing and social withdrawal.
Morgellons syndrome presents with non-healing sores and embedded fibers, but lacks medical evidence of infection.
Management of all these conditions requires a combination of antipsychotic medications, behavioral therapy, and dermatological care.

4
Obsessive-compulsive behaviour (OCB) is common in dermatology patients, with up to 25% prevalence.
Body dysmorphic disorder (BDD)
Lichen simplex chronicus
Nodular prurigo
Skin picking disorder
Acné excoriée
Trichotillomania
Onychotillomania and onychophagia
Health anxieties



4
Avoid dismissing patient concerns.
Encourage open discussion about compulsive habits.
Determine triggers such as:
Anxiety
Stress
Obsessive-compulsive disorder (OCD)
Do not say “it’s all in your head.”
Acknowledge the patient’s distress.


4
Cognitive-behavioral therapy (CBT) is effective.
May require specialized psychotherapist support.
Patients can learn self-awareness techniques.
Online resources and self-help materials may be useful.
4
SSRIs (Fluoxetine, Sertraline, Paroxetine) are first-line treatments.
Higher doses may be necessary (effects seen after 4–6 weeks).
Clomipramine and Doxepin can be alternatives.
Psychodermatology MDT (Multidisciplinary Team) management improves outcomes.
Address skin damage alongside psychological support.



4
Body Dysmorphic Disorder (BDD) is characterized by an obsessive preoccupation with an imagined or minor physical flaw.
Patients perceive a small or non-existent defect as severely disfiguring.
It has also been called Dysmorphophobia, though this term is now discouraged.
Prevalence: 1–2% of the general population.
Common in cosmetic surgery seekers.
Female:Male ratio ~2:1.
Onset typically occurs in adolescence.



4
Persistent intrusive thoughts about appearance.
Frequent mirror checking or mirror avoidance.
Skin picking, excessive grooming, and seeking reassurance.
Social withdrawal, depression, and suicidal ideation
(about 25% attempt suicide).

4
CBT (Cognitive Behavioral Therapy) is most effective.
SSRIs (Fluoxetine, Sertraline, Paroxetine) for reducing obsessive thoughts.
Atypical antipsychotics
(Risperidone, Aripiprazole) in severe cases.
Psychodermatology MDT referral for complex cases.



4
Lichen Simplex Chronicus (LSC):
Localized, thickened plaques caused by repetitive scratching or rubbing.
Nodular prurigo:
Generalized form with nodular lesions from chronic scratching.
Prevalence: 1–10%.
Peak age:
19 years (atopic group)
48 years (non-atopic group)
More common in women.
Slightly more frequent in Afro-Caribbean and Oriental populations.

4
Thickened, scaly plaques or nodules on easily reachable areas.
Persistent itching, often leading to lichenification.
Can be triggered by anxiety or OCD tendencies.



4
Topical steroids (Clobetasol, Betamethasone) under occlusion.
Oral antihistamines (Cetirizine, Hydroxyzine) for itch.
Gabapentin or Pregabalin for neuropathic itch.
Phototherapy (PUVA, narrowband UVB).
Psychotherapy (CBT) for compulsive scratching.


4
Skin Picking Disorder (Excoriation Disorder) is characterized by compulsive picking of normal or slightly irregular skin.
It is often associated with stress, anxiety, or body dysmorphic disorder (BDD).
It is also called Dermatillomania.
More common in females.
Often co-exists with OCD or depression.


4
Repeated skin picking leads to sores, scars, and infections.
Commonly affects:
Face
Arms
Scalp
May involve ritualistic behaviors.
4
CBT with habit reversal therapy.
SSRIs (Fluoxetine, Sertraline) to reduce compulsion.
N-acetylcysteine (1200–2400 mg/day) as an adjunct therapy.


4
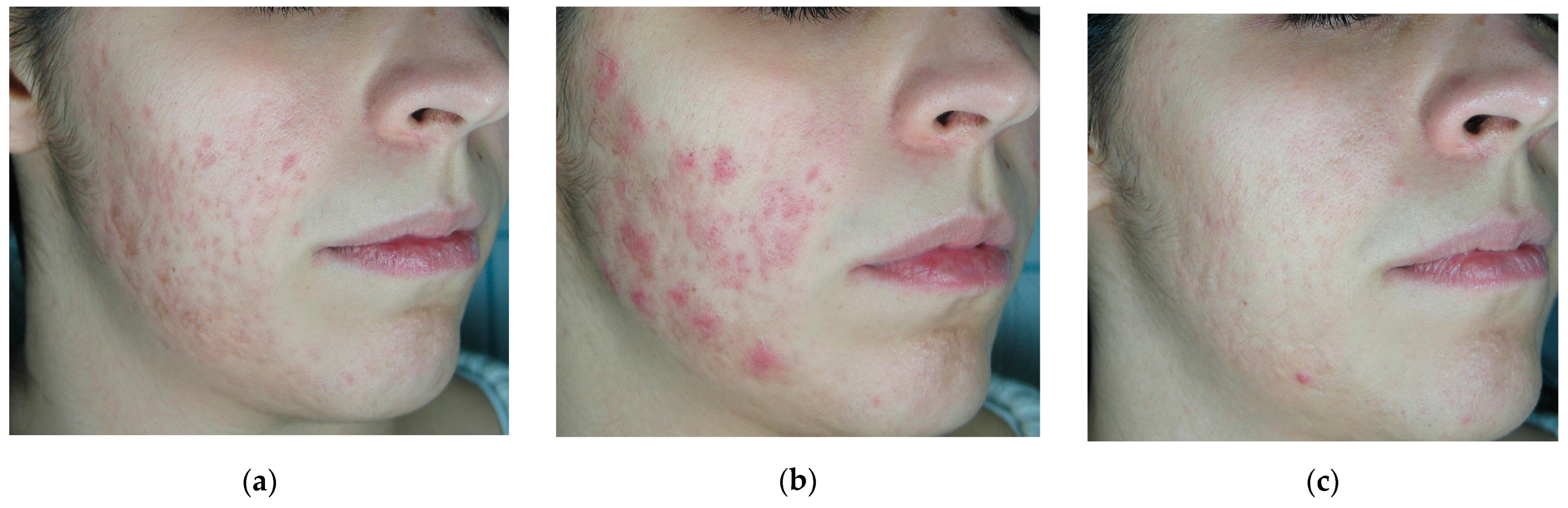
Acné excoriée is a type of compulsive skin picking disorder targeting acne lesions.
It affects individuals who continuously pick at acne, worsening the condition.
Common in young women with underlying anxiety or BDD.
Frequently associated with OCD spectrum disorders.


4
Excoriated acne lesions with post-inflammatory hyperpigmentation or scars.
Patients often feel compelled to “remove imperfections.”
Lesions heal poorly due to repeated trauma.


4
CBT and SSRIs (Fluoxetine, Sertraline).
Benzoyl peroxide or topical retinoids for acne management.
Low-dose Isotretinoin (controversial, used in select cases).
Habit-reversal therapy (HRT).
Obsessive-compulsive behaviors in dermatology involve chronic skin-damaging habits.
Psychological conditions like BDD, skin picking disorder, and acné excoriée require combined dermatological and psychiatric treatment.
CBT and SSRIs are the mainstay treatments for OCD-related dermatological conditions.
Multidisciplinary teams (MDT) significantly improve patient outcomes.

4
Trichotillomania (Hair-Pulling Disorder) is a behavioral disorder characterized by compulsive hair-pulling, resulting in noticeable hair loss.
The term was first used by Hallopeau in 1889 and comes from Greek:
Thrix – hair
Tillein – pull out
Mania – madness
It is more accurately classified as an OCD spectrum disorder rather than a true “mania”.
Recurrent pulling out of one's own hair, causing hair loss.
Increasing tension before pulling or attempting to resist the behavior.
Pleasure, gratification, or relief when pulling the hair.
Not explained by another mental disorder.
Causes significant distress or impairment in daily life.
Prevalence: 0.6–3%, more common in children and college students.
Two peaks:
Preschool children (2–10 years)
Often self-limiting
Adolescents and adults
Chronic and more severe cases
Childhood: Male > Female (62% boys)
Adolescents and adults:
Female:Male = 4:1 to 15:1

4
Considered an impulse control disorder with links to:
Obsessive-compulsive disorder (OCD)
Anxiety disorders
Depression
Familial predisposition has been reported.
May be triggered by psychosocial stress.
Hair loss affecting:
Scalp
Eyebrows
Eyelashes
Pubic area
Broken hairs of varying lengths with normal scalp skin.
Repeated pulling may lead to:
Scarring
Folliculitis
Secondary infections
Some patients eat the pulled hair, which may lead to trichobezoars (hairballs in the stomach).

4
Cognitive-Behavioral Therapy (CBT) with Habit Reversal Therapy (HRT).
Selective Serotonin Reuptake Inhibitors (SSRIs)
(Fluoxetine, Sertraline, Paroxetine).
N-Acetylcysteine (1200–2400 mg/day) for impulse control.
Mood stabilizers
(Gabapentin, Pregabalin).
Atypical antipsychotics
(Olanzapine, Risperidone) for severe cases.
Referral to a psychiatrist for severe or resistant cases.

4
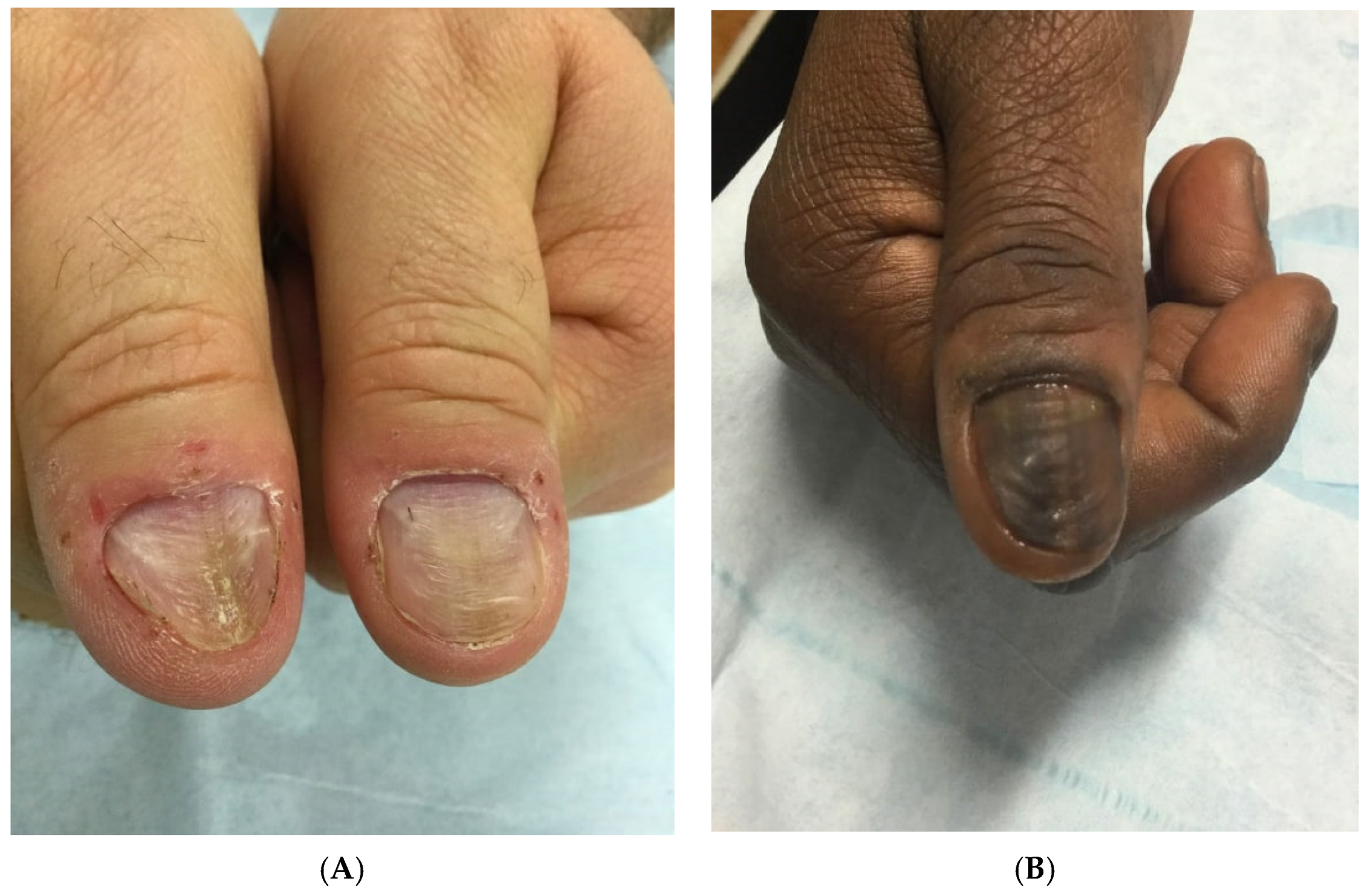
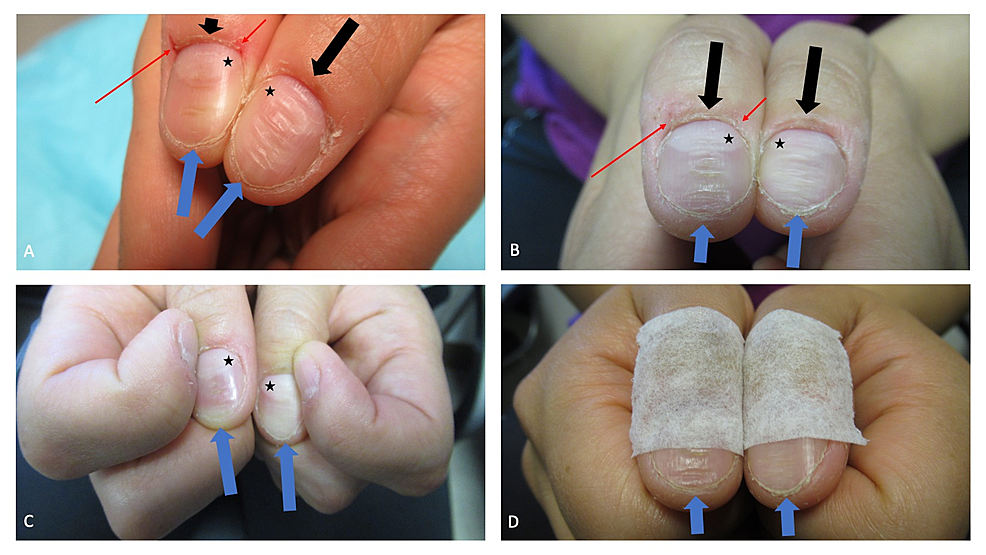
Compulsive picking or pulling of the nails or periungual skin.
Chronic nail biting behavior.
Both are considered body-focused repetitive behaviors (BFRBs) associated with OCD spectrum disorders.
Damaged nail plates.
Irregular or shortened nails.
Inflamed periungual skin.
Paronychia or infections due to repeated trauma.
Habit Reversal Therapy (HRT).
CBT for compulsive habits.
SSRIs when associated with OCD or anxiety disorders.
Protective nail coverings or bitter nail coatings to reduce biting.


4
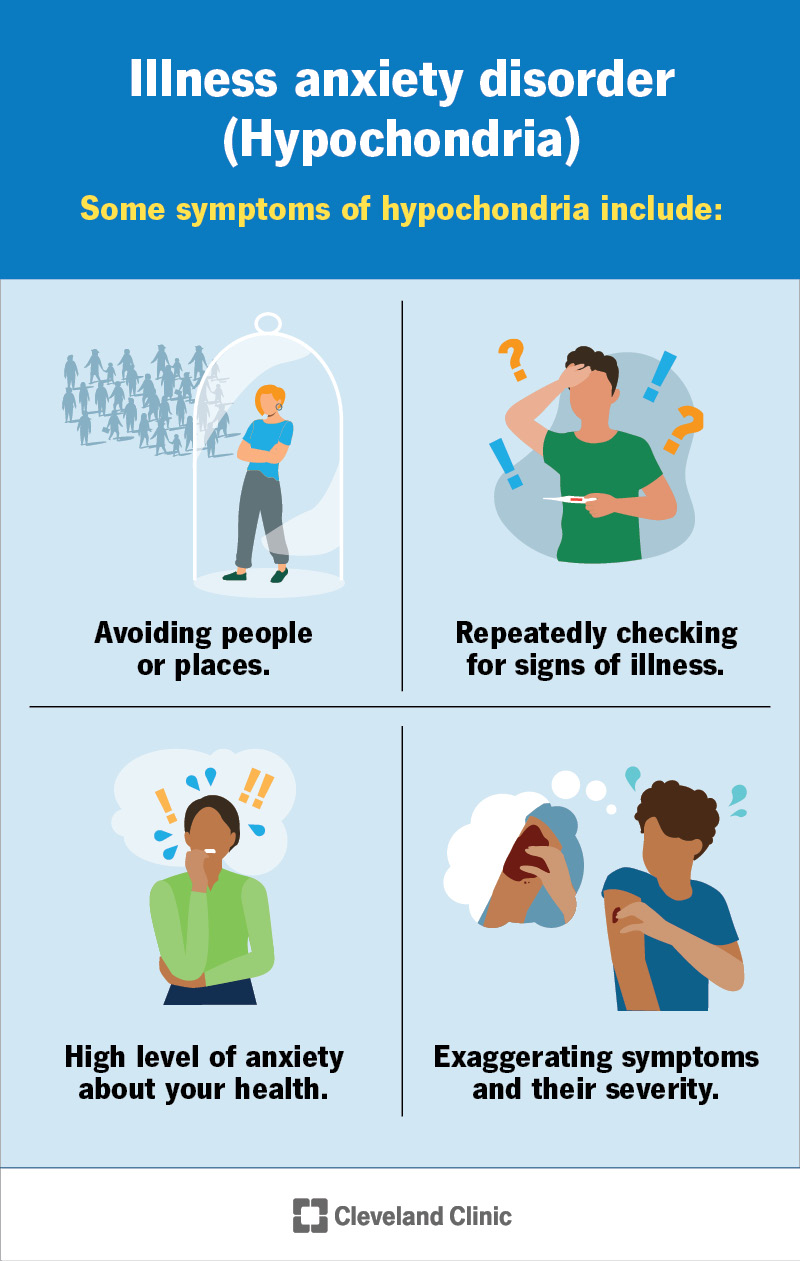
Health anxiety refers to excessive worry about having a serious illness despite medical reassurance.
In dermatology, patients may become fixated on minor skin changes, fearing serious disease.
Persistent concern about skin disease.
Repeated dermatology consultations.
Excessive self-examination of skin.
Misinterpretation of benign lesions as dangerous conditions.
Cognitive Behavioral Therapy (CBT).
SSRIs when anxiety is severe.
Provide clear explanations and reassurance.
Avoid unnecessary investigations that reinforce illness beliefs.
Trichotillomania involves compulsive hair pulling, leading to patchy alopecia.
Onychotillomania and onychophagia involve repetitive nail picking or biting.
Health anxiety leads to excessive worry about dermatological disease.
CBT, Habit Reversal Therapy, and SSRIs are the core treatments for many psychodermatological behavioral disorders.
4
Onychotillomania: Compulsive nail-picking.
Onychophagia: Compulsive nail-biting.
Both are body-focused repetitive behaviors (BFRBs) and can lead to:
Permanent nail dystrophy
Infections
Self-mutilation
Common in children and adolescents.
Nail-biting prevalence:
60% of children
45% of adolescents
10% of adults
More common in individuals with:
Obsessive-compulsive disorder (OCD)
Anxiety disorders
Impulse-control disorders

4
Nail deformities
Shortened nails
Transverse ridges
Irregular nail edges
Paronychia and secondary infections
Bacterial infections
Fungal infections
Bleeding and pain
Permanent nail dystrophy in severe cases.
Thumb-sucking
Hair-pulling (trichotillomania)

Cognitive Behavioral Therapy (CBT) with Habit Reversal Training (HRT).
Bitter-tasting nail polish to discourage biting.
Stress reduction techniques
Mindfulness
Relaxation therapy
SSRIs (Fluoxetine, Sertraline) for coexisting anxiety or OCD.
Local antiseptics and topical steroids for nail infections.
Oral antipsychotics (Pimozide, Risperidone) in rare severe cases.
Referral for psychiatric evaluation in self-harm cases.


4
Health anxiety is an irrational fear of developing a serious medical condition, also known as cutaneous phobias in dermatology.
Dirt phobia
Germ phobia
Wart phobia
Patients often wash their hands excessively, leading to:
Dermatitis
Skin damage
Cancer phobia
Mole phobia
Patients may:
Frequently request mole checks
Demand excisions or skin biopsies
Blushing phobia
Sweating phobia (hyperhidrosis concerns)
Topical steroid phobia (fear of skin thinning)
Persistent anxiety about various diseases despite reassurance.
Common in patients with:
Obsessive-compulsive disorder (OCD)
Hypochondriasis
Generalized anxiety disorder (GAD)
Often worsened by:
Family history of cancer
Family history of skin disease
Social media and misinformation can exacerbate fears.



4
Repeated doctor visits for reassurance.
Excessive self-examinations of the skin.
Compulsive online research about diseases.
Compulsive washing or avoiding sunlight due to fear of skin damage.
In severe cases, may develop delusional disorder, such as believing harmless lesions are cancerous.

4
Cognitive Behavioral Therapy (CBT) to challenge irrational fears.
Mindfulness and relaxation techniques.
Psychoeducation about skin health.
SSRIs (Fluoxetine, Sertraline, Citalopram) for severe anxiety.
Benzodiazepines for short-term use in acute anxiety episodes.
Antipsychotic medications (Olanzapine, Aripiprazole) in delusional cases.
Hypnotherapy and guided imagery for resistant cases.
Referral to a psychodermatology specialist for complex cases.
Trichotillomania is a compulsive hair-pulling disorder linked to OCD, stress, and anxiety.
Onychotillomania and Onychophagia involve compulsive nail-picking and biting, causing nail deformities and infections.
Health anxieties include irrational fears of skin diseases, leading to excessive medical visits and self-damaging behaviors.
CBT, SSRIs, and stress management are the core treatments for these psychodermatological conditions.

4
Eating disorders are primarily psychiatric illnesses with significant physical complications.
Anorexia nervosa
Bulimia nervosa
Eating disorders not classified
These disorders are most common in young women and are increasing in incidence worldwide.

4
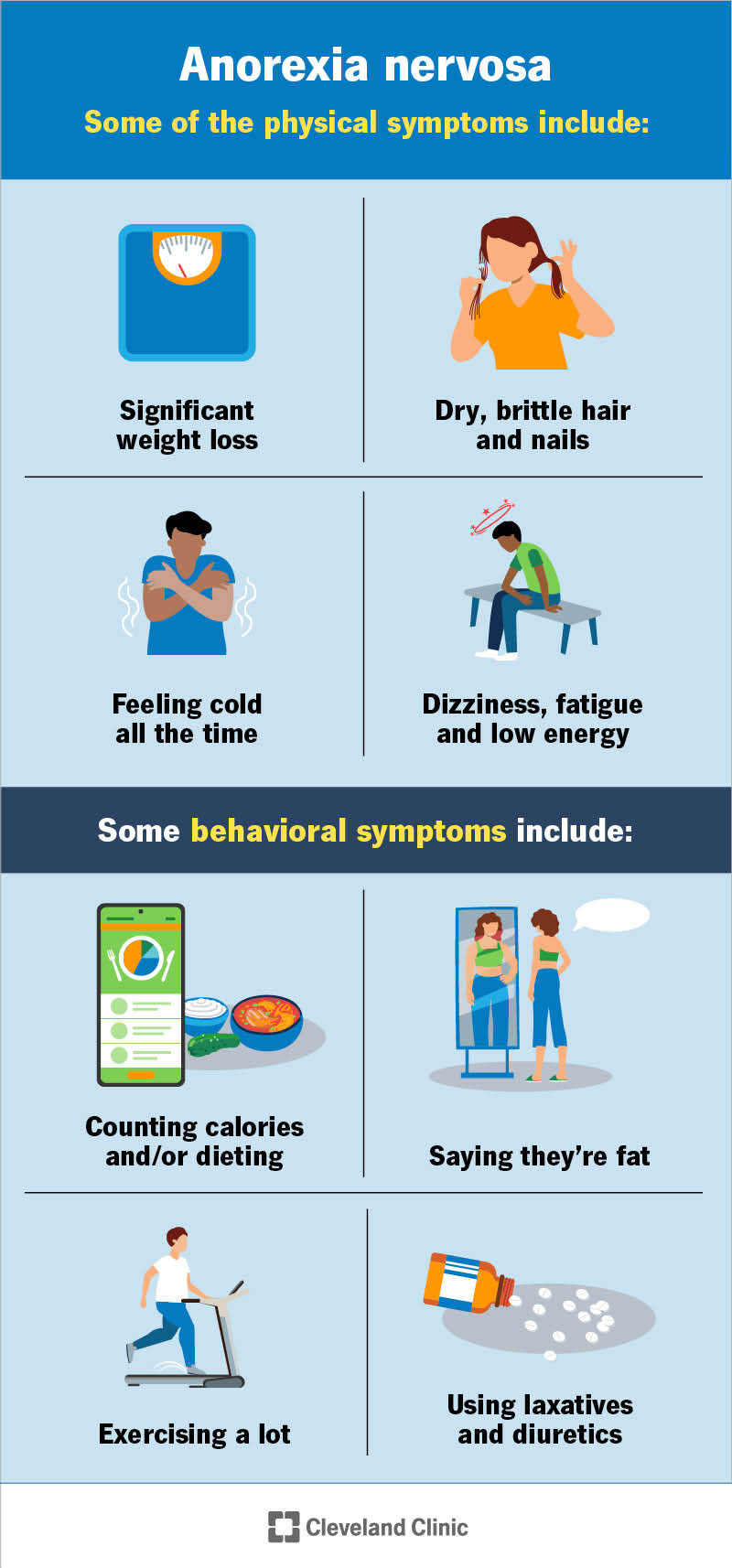
Anorexia nervosa is characterized by:
Inability to maintain a normal weight for age and height
(BMI <17.5 kg/m²)
Intense fear of gaining weight despite being underweight
Distorted perception of body weight and shape
Amenorrhea (absence of menstruation)
Incidence: ~1% of the general population
Prevalence: 0.3% annually
Peak age: Adolescence
Gender ratio:
Female:Male = 20:1, though recent trends suggest 5:1
Most common in white, industrialized societies

4
Severe weight loss
Cachexia (muscle wasting)
Bradycardia
Hypotension
Hypothermia
Lanugo (fine body hair growth) due to lack of fat insulation
Xerosis (dry skin) and pruritus
Pellagra (niacin deficiency)
Raynaud’s phenomenon and acrocyanosis (bluish hands/feet)
Hair loss or hypertrichosis
Russell’s sign (knuckle calluses from self-induced vomiting)

4
Bulimia nervosa is characterized by:
Recurrent binge-eating episodes (compulsive overeating)
Recurrent compensatory behaviors to prevent weight gain
Self-induced vomiting (most common)
Laxative abuse
Diuretic abuse
Binge eating and purging occur at least twice per week for 3 months.
Self-esteem is heavily influenced by body weight and shape.
Prevalence: Up to 5% of the general population
Annual prevalence: 1%
Peak age: Late teens to early twenties
Gender ratio: Female:Male = 20:1
More common in high socioeconomic groups
4
Normal or slightly low body weight (unlike anorexia)
Frequent vomiting leading to metabolic alkalosis
Enlarged parotid glands due to chronic vomiting
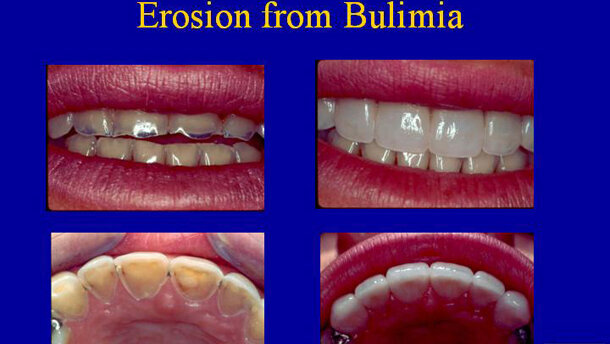
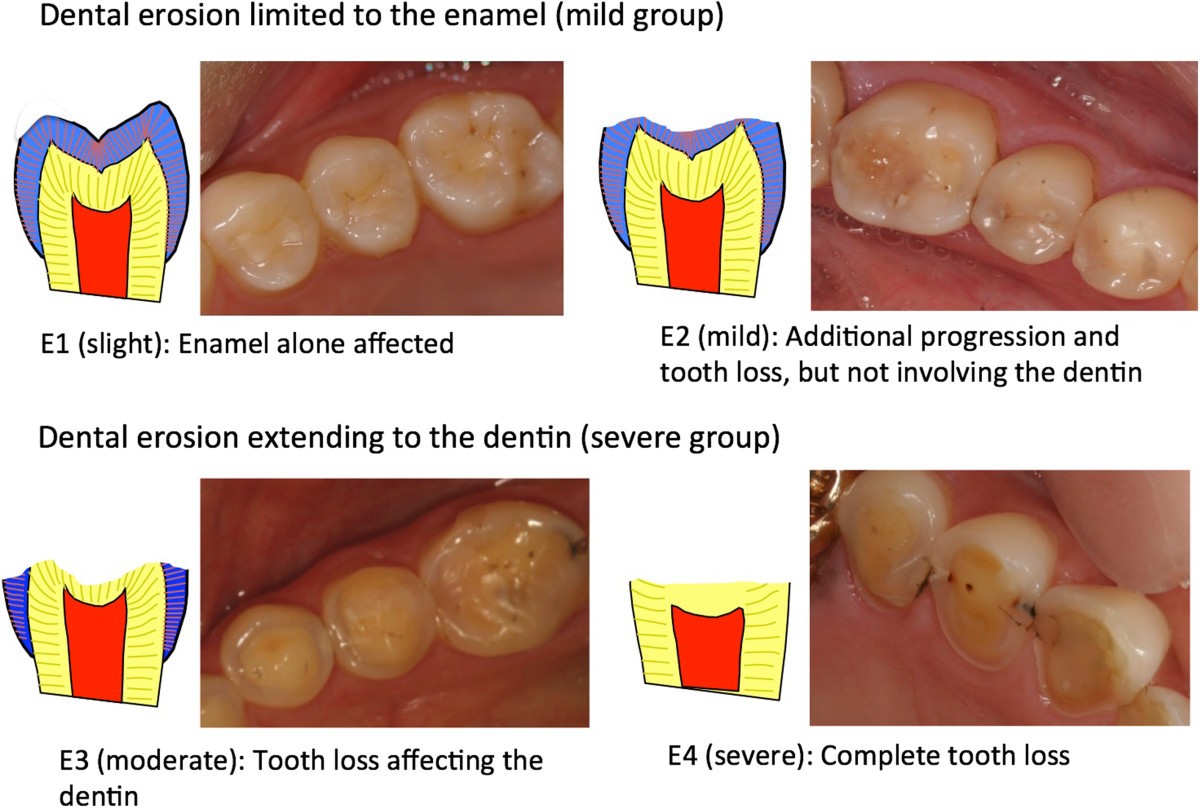
Dental erosions from stomach acid
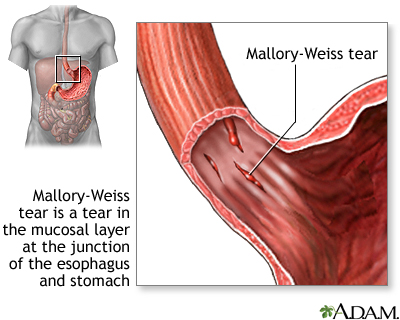
Esophageal tears (Mallory-Weiss syndrome)
Russell’s sign (knuckle calluses from repeated vomiting)



Fluoxetine (up to 60 mg/day) — FDA-approved for bulimia
Citalopram (up to 40 mg/day) for anxiety and OCD symptoms
Mirtazapine (if sleep disturbances present)
Best evidence for treating bulimia
Aims to change dysfunctional thoughts about food, body image, and weight
Supervised weight gain programs for anorexia
Correction of micronutrient deficiencies

4
Antipsychotics (Olanzapine, Risperidone) for severe weight gain resistance
Mood stabilizers (Lamotrigine) if bipolar disorder is present
Mindfulness and relaxation techniques



4
Hypnosis and alternative psychotherapies
Hospitalization for severe cases
(BMI <15 kg/m²)
Anorexia nervosa:
Extreme weight loss, fear of gaining weight, and amenorrhea.
Bulimia nervosa:
Binge eating followed by purging, normal body weight, and dental erosions.
Treatment:
CBT and SSRIs (Fluoxetine 60 mg/day for bulimia).
Severe cases require hospitalization to prevent life-threatening complications.


4
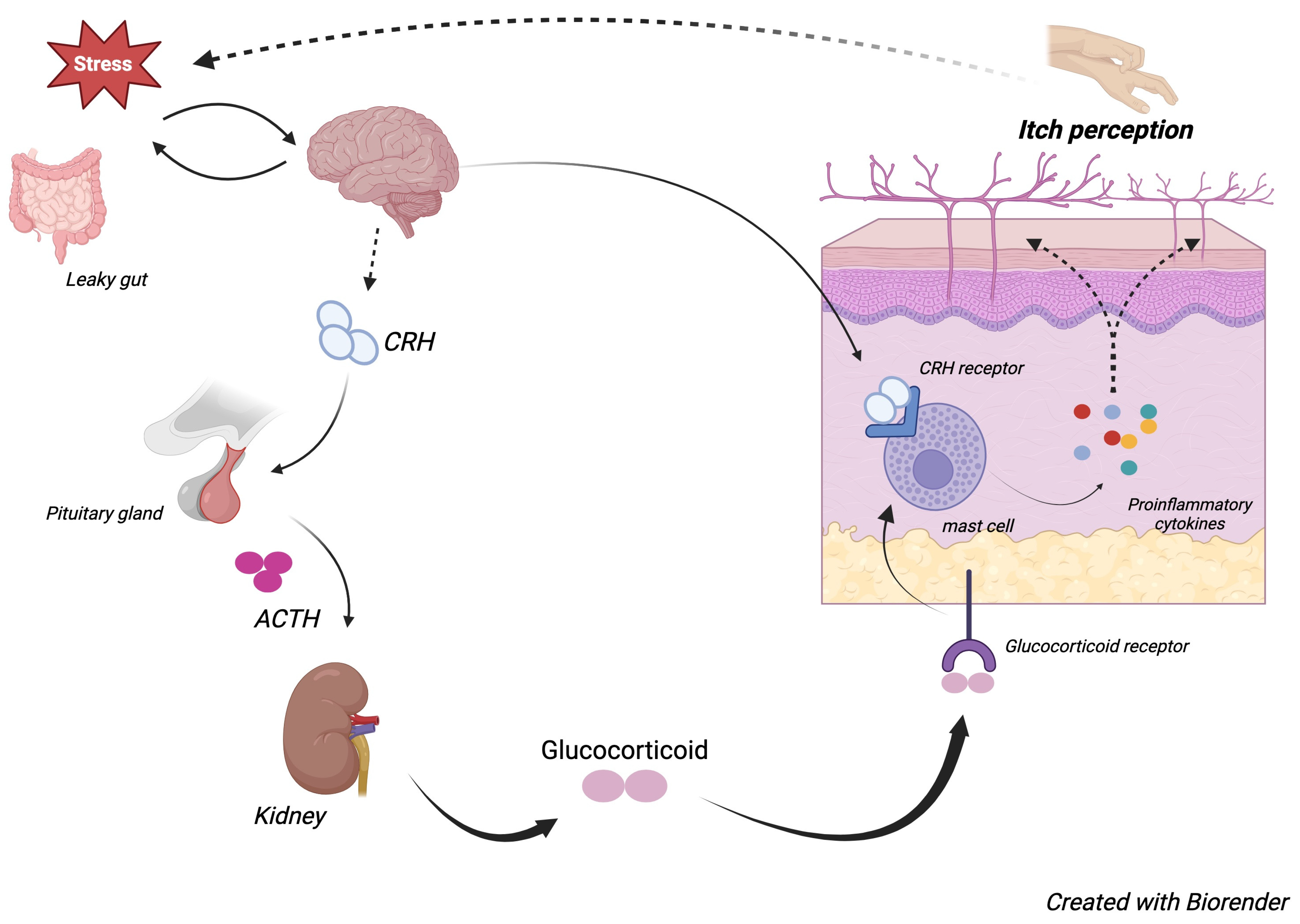
Psychogenic itch (psychogenic pruritus) refers to itching without a clear dermatological, systemic, or neurological cause.
It is classified under psychosomatic disorders and is commonly triggered or worsened by stress, anxiety, or psychiatric conditions.
Psychological factors can provoke or amplify the sensation of itch, even in the absence of actual skin disease.
Three compulsory criteria must be met:
Localized or generalized pruritus without an identifiable cause.
Chronic pruritus lasting more than 6 weeks.
Absence of any somatic (organic) disease explaining the symptoms.
4
Psychogenic pruritus often begins as a stress response.
Itching episodes may occur unpredictably, often at times of relaxation or mental distress.
Crawling sensations
Stinging sensations
Burning sensations
The itch is often localized initially but may generalize over time.
Common affected areas
Legs
Arms
Back
Some patients derive pleasure from scratching, possibly due to opioid release in the brain.

4
No visible skin disease at onset.
Excoriations, lichenification, and secondary infections can develop due to excessive scratching.
Unpredictable onset and resolution.
Frequently associated with:
Anxiety
Depression
Obsessive-compulsive traits
Nodular prurigo
Depression (~30% of cases)
Anxiety and depression
10% in outpatients
20% in inpatients

Treatment should address both the itch sensation and the underlying psychological condition.
Topical emollients
Mild corticosteroids
Antihistamines (Hydroxyzine, Cetirizine) for sedation and itch control
Tricyclic antidepressants (Amitriptyline, Doxepin) for nocturnal itching

Selective Serotonin Reuptake Inhibitors (SSRIs) for associated anxiety and depression
Paroxetine
Sertraline
Fluoxetine
Gabapentin or Pregabalin for neuropathic itch
Psychotherapy (CBT) to address stress and compulsive scratching

4
Mood stabilizers
Lamotrigine
Lithium
Referral to a psychodermatology MDT for specialized care
Habit-reversal therapy (HRT) for compulsive scratching behavior
Psychogenic itch is a chronic pruritus disorder without an underlying somatic cause.
Psychological stress and emotional factors trigger the itch sensation.
Diagnosis is based on exclusion of organic skin or systemic diseases.
Management includes:
Skin care
Antihistamines
Antidepressants
Psychological interventions

4
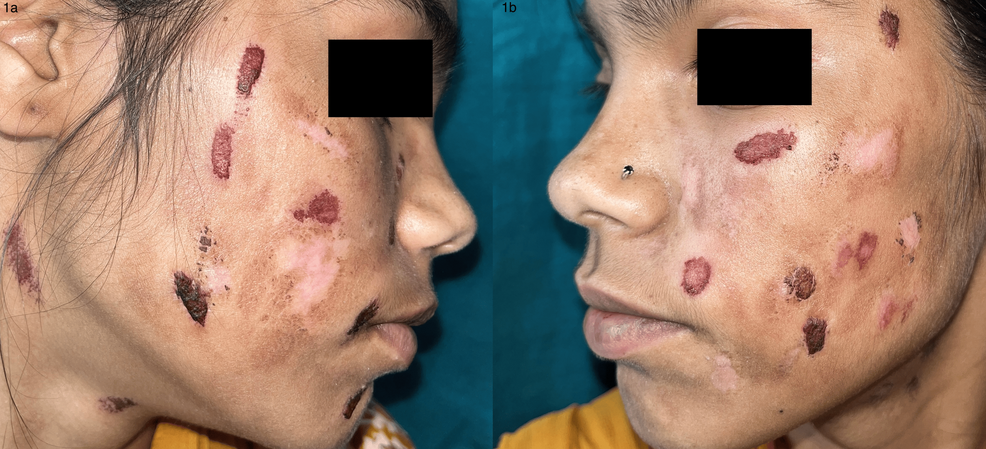
Factitious skin disease (FSD) refers to self-inflicted skin conditions where patients deliberately create lesions without an obvious external reward.
Lesions are intentionally self-inflicted.
Patients often deny or conceal their role.
No external gain
(unlike malingering, where compensation or avoidance of duty is the goal).
Dermatitis artefacta
Dermatitis simulata
Dermatological pathomimicry
Borderline personality disorder
Somatoform disorders
Depression
Anxiety

4
Dermatitis artefacta (DA) is a self-inflicted skin disorder in which patients cause lesions on their own:
Skin
Hair
Scalp
Nails
Mucosae
Patients deliberately conceal the cause from doctors.
More common in women
(Female:Male ratio 20:1 to 4:1)
Adolescence to early adulthood
Older onset in men
(Male:Female ratio 2:1)
4
Sudden onset of lesions without a clear history.
Lesions appear at the same stage of development, often symmetrical.
Face
Hands
Forearms
Lesions in hidden areas such as:
Breasts
Abdomen
Genitals
may suggest a history of abuse.
Linear patterns
Geometric patterns
Angulated patterns
Other manifestations include:
Erosions
Blisters
Burns
Ulcers
Hyperpigmentation
“Hollow history”
Patient cannot provide a clear explanation for the onset of lesions.
Psychodermatology multidisciplinary approach
Cognitive Behavioral Therapy (CBT)
SSRIs
Fluoxetine
Sertraline
for underlying anxiety and depression.


4
Atypical antipsychotics
Olanzapine
Risperidone
Habit Reversal Therapy (HRT).
Referral to psychiatry if:
Comorbid personality disorder
Severe self-harm
Factitious skin disease involves intentional self-inflicted skin lesions without external reward.
Dermatitis artefacta is the most common form.
Characteristic features include:
Geometric lesions
Symmetrical patterns
“Hollow history.”
Management requires psychodermatology collaboration, combining dermatologic care and psychiatric treatment.


4
Dermatitis simulata refers to a condition in which patients mimic a skin disease using external materials such as makeup, glue, dyes, or chemicals.
Unlike dermatitis artefacta, no true skin damage occurs.
Fake rashes, scars, or ulcers created using cosmetics or irritants.
Makeup may be used to simulate vascular lesions.
Glue, sugar, or dyes may be applied to create the appearance of:
Scaling
Blisters



4
Simple cleaning with water or alcohol removes the simulated lesion.
Lack of histological findings supports the diagnosis.
Gentle confrontation without accusations.
Cognitive Behavioral Therapy (CBT) and supportive psychotherapy.
SSRIs for underlying psychiatric conditions.


4
Dermatological pathomimicry occurs when a patient intentionally worsens an existing skin disease.
Unlike dermatitis artefacta, these patients exacerbate a pre-existing condition rather than create a new one.
Delayed healing of surgical wounds due to intentional interference.
Exaggeration of skin reactions following minor trauma.
Recurrent unexplained flares of chronic skin diseases such as:
Psoriasis
Eczema

4
Skin biopsy may show evidence of external manipulation.
Close monitoring and controlled treatment can reveal recurrent manipulation patterns.
Cognitive Behavioral Therapy (CBT).
Habit Reversal Therapy (HRT).
SSRIs or mood stabilizers in resistant cases.
Supervised skin care with clear treatment protocols.
Factitious skin disease involves intentional self-inflicted skin lesions without external rewards.
Dermatitis artefacta:
Self-inflicted skin damage, often hidden from doctors.
Dermatitis simulata:
Imitation of skin disease without actual damage.
Dermatological pathomimicry:
Intentional worsening of an existing skin disease.
Management requires a psychodermatology MDT, including:
CBT
Supportive psychotherapy
SSRIs or antipsychotics when needed
Get the full PDF version of this chapter.